








Liz Stevenson started her day at 5:30 a.m. with a cup of tea and a crossword puzzle. She got in a workout and had a conversation with her husband, Richard, over coffee before getting into her silver minivan and heading to work — where she was going to help someone die.
Stevenson, a youthful 58, is a hospice nurse, a visiting nurse for Holy Redeemer Home Care and Hospice. There are three kinds of nurses in the medical world: those at the beginning, middle and very end of our lives. Hospice nurses, like Stevenson, are part of a rapidly growing sector of health care that provides medical services at the end of someone’s life.
On this Monday, Stevenson is visiting the Kozior home in Somers Point. The ranch home has a screened-in porch and a newly built wooden ramp at the front door.
Stevenson, sitting on a hospital cot in the homey living room, applies a pressure cuff to the arm of Stan Kozior and gently uses her stethoscope to listen to his heart. Stevenson’s soothing tone and calming nature come through as she talks to her patient and his wife, Phyllis.
People are also reading…
Stan, 90, smiles at her from his chair. Stevenson has been coming to the home since January, and he is comfortable enough with her to serenade her with an old Polish song. Stevenson smiles back and holds his aged hands between hers. “This is why I love coming here,” she said.
Stevenson has gotten to know the Koziors. She knows they have been married for nearly 43 years. She knows their children’s ages, and she knows the names of the grandchildren in the photos that overwhelm a side table.
She also knows Stan is dying of renal failure and dementia. It is a tough reality. Especially for Phyllis.
“We did everything in our marriage together. We’ve always done everything together,” Phyllis said. “When the doctor recommended hospice, it was hard. I realized that one day I will lose him. But this makes him happy, to be home.”
* * *
Stevenson is part of a team of doctors, social workers, pharmacists, volunteers and home health aides who make it possible for Stan to choose to die at home.
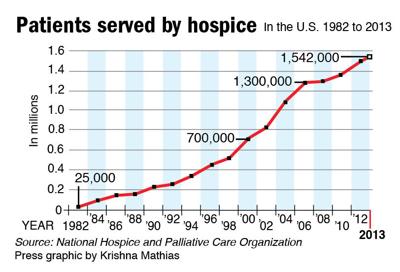
The number of people using end-of-life services has increased dramatically in recent years. The National Hospice and Palliative Care Organization estimates more than 1.5 million Americans accessed hospice care in 2013.
But aid-in-dying measures are still relatively new. Medicare did not cover hospice services until 1982, and the first hospice house in the U.S. for children didn’t open until 2003.
In the 1970s, there were few services to help an ill person die comfortably at home. That’s when Stevenson first saw what a difference end-of-life care could make.
Stevenson was barely out of her teens when she had to watch her Aunt Nancy, who was like a second mother to her, die of pancreatic cancer at age 49.
One blistering hot summer day Stevenson’s uncle sent her to refill a prescription for morphine for her aunt.
Back then, not all pharmacies carried morphine, she said. Stevenson walked from store to store, hoping someone would be able to fill the prescription, while her aunt lay at home in discomfort.
“I remember being in tears, saying, ‘I can’t get this,’” she said. There was only so much a 21-year-old could do.
Soon after, her uncle hired a licensed practical nurse to help the family. Stevenson said the nurse took over medical responsibilities so that the family could simply spend time with her aunt.
“She was a calming force, and you’re anything but calm when you’re watching someone suffer,” she said. The nurse provided personal care, delivered medications and comforted the family. “That was the first time I became interested in nursing.”
* * *
On her first day as a hospice nurse, Diane Alberto, of Northfield, came home crying.
She had been trying to help an elderly wife care for her husband, who had dementia.
“I felt so sad for what she was going through, how her whole life was turned upside-down. All I could think of was the life they used to have,” she said.
Eventually Alberto learned to cope with the emotions of the job, in part by leaning on Stevenson, whom she called her go-to girl for help and advice.
Alberto, Stevenson and other nurses in the hospice program meet at work regularly to support each other. Alberto said she admires the way Stevenson stays composed with families and knows exactly what needs to be done.
But it wasn’t always like that, Stevenson said.
“At one of the first meetings we had, everybody started off by talking about the patients they had lost,” she said, “and I just sat there and cried. My director was probably looking at me and thinking, ‘She’s not going to make it a week.’”
But Stevenson stayed with it, relying on the knowledge that her patients are cared for by an entire team of people.
“For the older patients, it’s more like a celebration of life,” she said. Caring for the younger patients is the hardest. Stevenson’s youngest patient was 26 years old, just one year younger than her own son, she said. “I can’t imagine going through that as a parent.”
Despite the serious nature of their work, both Stevenson and Alberto said they love their jobs.
“People ask, ‘How can you do this?’” Alberto said. “I feel special doing this because a lot of people simply can’t. Some nurses go in with a curative mindset, and it’s not about that. You’re doing the opposite. It’s about comfort and care, talking to a patient about their end-of-life wishes and how they want to go about it.”
* * *
Gallup polls show nearly 90 percent of adults would prefer to die at home, surrounded by loved ones and free of pain. In reality, only a fraction of people die this way.
Some doctors are so focused on curing patients — even at the end of terminal illnesses — they don’t take full advantage of end-of-life care. And many people have misconceptions about what hospice involves, said Christopher Bolich, doctor and medical director at Holy Redeemer. They think it means giving up.
When Phyllis Kozior told her friends she was going to use hospice care for Stan, they told her hospice would “ruin everything.” But that’s not what happened, Phyllis said, as she continued to get support from Stevenson and a hospice team.
“They give me so much help. I would have been lost.”
Before becoming a hospice nurse, Stevenson worked in medical and surgical units at a hospital. It was a fast pace, a blur of faces and concerned families.
She didn’t have time to hold anyone’s hand. She really didn’t know very much about her patients’ lives outside their illnesses.
“There are things you have to do, things you should do and things that would be nice to do,” Stevenson said. “In hospice, you get to do the nice things. It’s great to walk into situations and have the ability to make a difference, to provide the services they need.”
Sometimes, in addition to performing medical exams and recommending medications, those services involve just listening.
“One thing I really enjoy is that everyone has a story,” Stevenson said. “They want to share their story.”
Now, when Stevenson spends time outside work playing cards with friends, going to the beach with her family or seeing her grandson, she knows she is making stories of her own, stories she can share when her time comes.
“When you work with dying patients, you hit the realization that it’s going to be you one day,” she said. “It changes the way you go through life, and it’s bittersweet. I sometimes wish I didn’t think about it 24/7, but on the other hand, it makes life more enjoyable.”







{kind=link}
Welcome to the discussion.
Keep it Clean. Please avoid obscene, vulgar, lewd, racist or sexually-oriented language.
PLEASE TURN OFF YOUR CAPS LOCK.
Don't Threaten. Threats of harming another person will not be tolerated.
Be Truthful. Don't knowingly lie about anyone or anything.
Be Nice. No racism, sexism or any sort of -ism that is degrading to another person.
Be Proactive. Use the 'Report' link on each comment to let us know of abusive posts.
Share with Us. We'd love to hear eyewitness accounts, the history behind an article.