Abstract and Introduction
Abstract
Asthma is often associated with various comorbidities. The most frequently reported asthma comorbid conditions include rhinitis,
sinusitis, gastroesophageal reflux disease, obstructive sleep apnea, hormonal disorders and psychopathologies. These conditions
may, first: share a common pathophysiological mechanism with asthma; second: influence asthma control, its phenotype and response
to treatment; and third: be more prevalent in asthmatic patients but without obvious influence on this disease. For many of
these, how they interact with asthma remains to be further documented, particularly for severe asthma. If considered relevant,
they should, however, be treated appropriately. Further research is needed on the relationships between these conditions and
asthma.
Introduction
Asthma is a common airway inflammatory disorder characterized by variable airway obstruction and hyperresponsiveness.[301] Asthma is of variable severity and is increasingly recognized as a condition presenting as various phenotypes.[1,2] Asthma control is the main goal of therapy and is achieved when the disease results in minimal or no symptoms, normal sleep
and activities, and optimal pulmonary function.[3,4] Such control can be obtained with patient education, avoidance of environmental triggers, individualized pharmacotherapy
and regular follow-up.
Numerous comorbidities can be associated with asthma and influence its clinical expression, although their specific influence
remains to be characterized. They are, however, increasingly recognized as important factors to document in asthma patients
as they may influence disease management and control.
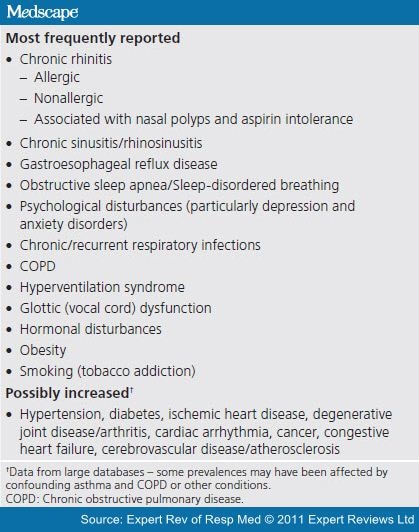
Among the most frequently contributing comorbid conditions reported in asthmatic patients are rhinitis, sinusitis, gastroesophageal
reflux disease (GERD), obstructive sleep apnea (OSA), hormonal disorders and psychopathologies, although other conditions,
sometimes without an evident link with asthma, have been found to be highly prevalent in asthmatic patients (Figure 1).[5,6] Indeed, analyses of large databases have shown an increased prevalence of a variety of conditions in asthmatic patients,
which either influence or do not influence asthma outcomes. These large-scale analyses may, however, be biased due to contamination
with, for example, patients with chronic obstructive pulmonary disease (COPD) or other conditions (
Box 1
).
Figure 1.
 Enlarge
EnlargeSome Common Asthma-related Comorbidities. ABPA: Allergic bronchopulmonary aspergillosis; COPD: Chronic obstructive pulmonary
disease; GERD: Gastroesophageal reflux disease; OSA: Obstructive sleep apnea. Reproduced with permission from199. © European Respiratory Journal.
In one of those reports, Prosser et al. used cross-sectional health services administrative data on treated adult asthma patients and on the general population
from British Columbia (Canada), using a standardized comorbidity identification methodology, the Adjusted Clinical Group Case-Mix
System.[5] Adults with asthma had significantly more comorbidities than the general population, such as respiratory infections, allergic
rhinitis and high impact/high prevalence chronic conditions such as depression, found in one out of four adults with asthma.
Children with asthma had a lower comorbidity burden than adults, but 12.6% had an associated chronic medical condition.
Gershon et al. used health administrative data of 12 million residents of Ontario, Canada, in 2005, to look at comorbidities associated
with asthma, as reflected by hospitalizations, emergency department visits and ambulatory care claims.[7] Asthma was associated with increased comorbidities, resulting in increased healthcare use, decreased quality of life and
poor asthma control.
Soriano et al. estimated the prevalence of comorbid diseases from an administrative data-based study including 7931 patients with asthma
and matched controls.[6] The most prevalent associated condition in adult asthmatic patients was time-limited minor infections while others with a
high impact and/or high prevalence were depression, hypertension, diabetes, ischemic heart disease, degenerative joint disease,
cardiac arrhythmia, cancer, congestive heart failure, cerebrovascular disease and COPD. A total of 60% of adult asthma patients
had at least one condition, and 12% had three or more. They also found an increased prevalence of comorbidities including
various respiratory, cardiac and neurological conditions, injuries and poisonings, in individuals with asthma compared with
those without asthma.[6] In both COPD and asthma, the total sum of diagnoses associated with 23 major organ systems was higher than in their matched
population controls. Among incident asthma patients, the occurrence of events was generally lower than in COPD, possibly due
to the younger age distribution, except for respiratory infection, but also probably due to the different impact of the disease
on various systems and to the presence of common risk factors such as smoking.
In a report by Adams et al., patients with asthma had an increased prevalence of diabetes, arthritis, heart disease, stroke, cancer and osteoporosis.[8] Van Manen et al. used a questionnaire in patients from 290 general practices over 40 years of age with asthma and/or COPD and 421 control
patients.[9] Musculoskeletal conditions, insomnia, stomach and duodenal ulcers, migraine, sinusitis, depression, cancer and atherosclerosis
were significantly more prevalent when patients had a diagnosis of asthma and/or COPD compared with controls. In an Australian
general population health survey performed by Adams et al. on 834 adults with asthma (6609 without), arthritis, heart disease, stroke, cancer and osteoporosis were more prevalent
in the presence of asthma, after age and sex adjustments.[8]
Finally, more recently, Cazzola et al., looking at data from the Health Search Database of the Italian College of General Practitioners, reported that asthma was
weakly associated with cardiovascular and hypertensive diseases;[10] surprisingly, the odds ratio of acute or past myocardial infarction was 0.84 (95% CI: 0.77–0.91). Furthermore, although asthma was weakly associated with depression, diabetes mellitus, dyslipidaemia, osteoporosis and rhinosinusitis, it was strongly associated with GERD and allergic rhinitis. There was no influence of age on the association of asthma with comorbidities.
In this article, we will further describe the relationships between asthma and its main associated comorbid conditions, particularly
those with a potential or established influence on asthma control.



;)